

Assumptions about Eating Disorder Behaviors
Eating disorders are a choice
In a short answer… No!
In a longer, more detailed answer, still no, but because eating disorders are complex ,biopsychosocial illnesses, meaning that there are biological, psychological, and social-environmental factors that ALL contribute to developing an ED, personal choice not being one of them. For some people, their eating disorder developed after a conscious attempt to change their diet or exercising patterns, but then became obsessive. Eating disorders are life-consuming, and can quickly end up having all the say in your personal choices. Here are some examples of biological, psychological, and social-environmental predisposition factors for eating disorders:
Biological Risk Factors:
- Having a close family member with an eating disorder/other mental illness
- Abnormalities in the structure and activity of the Hypothalamus
- Genetics
Psychological Risk Factors:
- Body image dissatisfaction
- Low Self-Image/Self-Esteem
- History of anxiety disorder, OCD, bipolar disorder, substance use, and other co-occurring disorders
- Perfectionism
- PTSD
Social-Environmental Risk Factors:
- Experience of bullying
- History of dieting
- Fatphobia/Weight Stigma
- Limited social networks
- Acculturation
- Intergenerational trauma and other traumatic experiences
Eating disorders are all about the food
People with eating disorders often engage in behaviors that have to do with manipulating their relationship with food, BUT eating disorders involve much more than that. Focusing heavily on using ED behaviors that impact body image and food is a tool to try to control aspects of their life where they feel they have no control. People use them as emotional tools, and overtime, can become the only thing that people rely on. Keeping up with an eating disorder is a lot of work! With all the time spent on them, they are often closely tied to one’s self-worth and perception, and it can be really hard for someone struggling to differentiate their identity and personal wants from that of the eating disorder. Telling someone with an eating disorder to “just eat” or “just stop eating” belittles their experience down to the most obvious part of their illness! People need to learn beneficial coping skills and receive support in all of the areas they’re struggling, not just the food part.
Everyone has an eating disorder these days
Disordered eating is HIGHLY common in our current society because there’s such a huge (and dangerous) emphasis on food and weight. The diet industry is worth a whopping $72 BILLION for pete’s sake! However, it’s untrue that everyone has an eating disorder, and saying so makes eating disorders, seem like a non-problem. Eating behaviors fall on a spectrum, from intuitive eating to eating disorder (see Fig. 1 for spectrum graph). Disordered eating and eating disorders can often be really hard to differentiate, as many diets and diet industry beliefs mimic eating disorder behaviors! Researchers estimate that 45 million Americans go on a diet each year, and while eating disorder prevalence is less, at 9% (~28.8 million people), dieting and disordered eating are strong precursors to developing an eating disorder. Researchers estimate that about 25% of people who diet later develop eating disorders (Shisslak, et. al., 1995). When a majority of people are subjected to, and by default, participate in fad diets and weight-loss ways of living, disordered eating becomes the norm, and nobody deserves that.
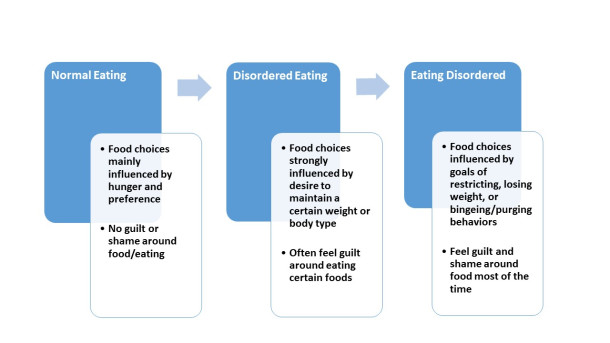
Figure 1. Spectrum of eating behaviors.
People experience just one type of eating disorder
Many people (Joy Project Team included) experience a continuum of eating disorder behaviors within and over the course of their illness. We can fluctuate between behaviors and symptoms that can crossover into multiple clinical diagnoses in what is often referred to as the “Eating Disorder Cycle” (Fig. 2). Longitudinal studies discovered that 73% of people with the initial diagnosis of Anorexia Nervosa had crossover during their lifetime (Gurze, 2008). This can be incredibly hard information to hear when a particular diagnosis can greatly impact and validate what someone with an ED is going through. But, this common experience of crossover means solely that the DSM is too rigid and tries to put eating disorders in a one size fits all box! The DSM does not reflect any of the complexities of this illness nor the people that experience them.
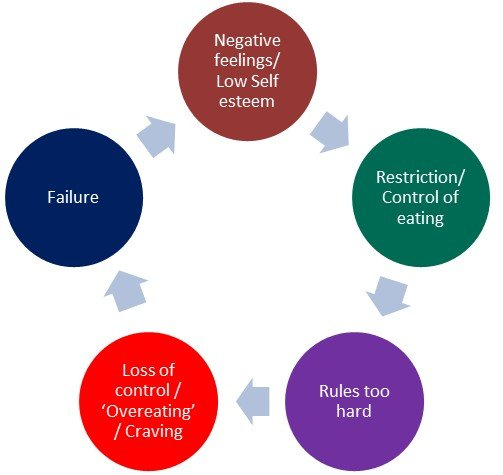
Figure 2. Example of the “Eating Disorder Cycle”
Eating Disorders aren’t serious
Eating Disorders are among the deadliest psychiatric illnesses, only second to that of Opioid use disorders (Arcelus, et. al., 2011). 10,200 deaths each year, or one death every 52 minutes, are due to eating disorders (Deloitte, 2020). This is often a direct result of both the medical complications that can come with an eating disorder and the mental strain eating disorders can put on a person. ~26% of people with eating disorders attempt suicide, and cardiovascular complications contribute to ~75% of people who die from eating disorders (Arcelus, et. al., 2011).
If you’re aware you have a problem, it’s probably not an eating disorder
It can take a ton of bravery and vulnerability to admit you’re struggling with an eating disorder. While it is true that people with eating disorders often try to keep their eating disorders and the behaviors they use a secret, it’s often not because they’re in denial. Eating disorders often thrive in secrecy, and can make the person suffering feel as though the eating disorder is the only thing that understands them and the stress they’re dealing with in everyday life. Similarly, just because someone admits that they have an eating disorder does not mean that they no longer need support. Admitting you have a problem is often just the first step!
Assumptions About Physical Appearance
Eating Disorders have a “look”
You can’t tell someone has an eating disorder by looking at them because eating disorders don’t have a LOOK! People with eating disorders come in all shapes and sizes. We call this myth size stereotyping, and it is a product of fat phobia and weight stigma! People with eating disorders often engage in a variety of behaviors that may or may not affect their weight and physical appearance. Size stereotyping, unfortunately happens far too often with eating disorders, and it’s a dangerous practice for a ton of reasons! Medical professionals who express weight bias might not recognize the severity of an eating disorder; friends and family members may not recognize problematic eating/exercising behaviors as disordered; insurance companies will often measure recovery, and the coverage they’re willing to give, by weight changes; someone struggling may not believe they have an eating disorder, or that their illness is not severe enough to warrant care!
Your eating disorder is only serious if you’re emaciated
The media loves to portray people with eating disorders in their most dramatic form to push a narrative that gets ratings. But this is not reality! Less than 6% of people with eating disorders are medically diagnosed as “underweight” (which is an arbitrary measure ANYWAY) (Arcelus, et al., 2011). Loved ones, medical professionals, and media perpetuating this assumption invalidates the experience of someone suffering with an ED and makes them believe they aren’t “sick enough” to have their illness taken seriously. Engaging in ANY eating disorder behaviors is serious.
Anorexia is the only serious eating disorder
All eating disorders are dangerous and can be life threatening. All. Of. Them. However, Anorexia often gets conflated as the most serious eating disorder, and often, the only one that requires a higher level of care. In a study performed in 2019, researchers used qualitative analysis to assess character traits and emotions that former eating disorder patients associated with their and their peers’ diagnoses (Mortimer, 2019). They found that participants associated Anorexia with virtues like self-control and strength, while Bulimia and Binge Eating were associated with traits like laziness and lack of self-discipline (2019). But NONE of this is true! ALL eating disorders are a maladaptive tool to cope with stressors, and NONE of them are determinants of moral value.
And it is not your fault if you yourself have believed this myth to be true. This idea is prevalent everywhere: Movies about eating disorders more often than not depict thin, white women from affluent, but highly-dysfunctional families, who get thinner as their ED grows; thinness is praised socially and is often conflated with anorexia; Weight stigma, fat phobia, and size stereotyping plays a major role in how eating disorders are viewed. What is important to remember is that this myth hurts everyone involved. It creates competition and pressure to conform to eating disorder behaviors and dieting practices in hopes to fit the thin ideal, which prevents people from seeking the help that they actually need and deserve.
Eating Disorders are ALL about vanity
NOPE! And even if they were… who cares? Plastic Surgery is a revered medical profession which success relies heavily on people’s vanity! People believe eating disorders are all about vanity because many of the visible eating disorder behaviors involve manipulating food and exercise. What may appear on the outside as vanity is actually someone’s detrimental attempt to cope, or disengage, with overwhelming thoughts and experiences going on in life. Those don’t go away simply by avoiding the mirror, nor does taking away the mirror magically make other, healthier coping mechanisms appear. Eating disorders stick around because they serve a purpose: they may continue to bring comfort, or at least an illusion of comfort, and may make life stressors seem more manageable. They may serve a purpose to help assuage anxiety around food fears. And often eating disorders persist out of deep rooted fear of being rejected or bullied for not fitting the beauty ideal.
Assumptions About Who Can Have an Eating Disorder
Eating disorders are a “girl” thing
Roughly 10 million men in America will experience an eating disorder sometime in their lifetime, but often won’t seek treatment or professional help due to the stigma associated with femininity and eating disorders (Strother, et. al., 2012). And unfortunately, most eating disorder treatment models are catered toward straight, white women. Eating disorder diagnosis, then, can often go overlooked in men due to how they may present. Fitness and sport can mask eating disorder behaviors in people participating. People in the LGBTQ+ community face unique challenges that put them at greater risk for eating disorders. Stigma, harassment and discrimination, insurance barriers, disphoria, and societal pressures and perceptions are all elements that particularly affect the LGBTQ+ community AND are linked to higher rates of eating disorders (Muhlheim, 2020). Eating disorders can affect anyone and everyone, and we have to have resources that reflect that.
Eating disorders are a teenage phase, they’ll grow out of it
Eating disorders are NOT a phase! This assumption poses HUGE dangers. Assuming this is just a phase negates any possibility of early intervention for kids who may be predisposed to developing an eating disorder. Early intervention is wildly beneficial in preventing prolonged harm and improving recovery outcomes! This assumption also pushes the idea that eating disorders only impact teenagers, which is so invalidating! Adults of any age can and do have eating disorders, but are pushed to the side with the belief that this illness is something someone can grow out of. Similarly, different developmental life stages can pose different triggers that may make the eating disorder rear its ugly head again. Everyone deserves validation, compassion, and support when they are struggling with something as devastating as an eating disorder, no matter their age.
Eating Disorders only affect white people
For all of recent history eating disorders have been conflated with thin, white women. Movies, celebrities, eating disorder treatment pamphlets all drive home this message that white women are the only people that get eating disorders, and especially are the only ones that get SERIOUS eating disorders. But this is NOT the case. Eating disorders disproportionately impact BI&POC and can be particularly violent due to added elements like acculturation and discrimination that contribute to them. Researchers reported recently that Black teenagers are 50% more likely than their white peers to exhibit behaviors consistent with Bulimia and Hispanic teenagers are also significantly more likely to exhibit Bulimia than their non-Hispanic peers (Deloitte, 2020). However, due to this false assumption, BI&POC with eating disorders are taken less seriously. BI&POC are significantly less likely than white people to be asked by a doctor about their eating disorder symptoms (Becker, et. al., 2003) AND half as likely to be diagnosed with an ED or receive treatment (Deloitte, 2020). Medical Professionals are not even immune to these myths and in fact, are in the most precarious of positions to be upholding such dangerous assumptions.
Assumptions About ED Recovery
Treatment is only for people in thin bodies
It really seems this way, doesn’t it? And that sucks. The thin ideal creates a nasty hierarchy in and out of the eating disorder community. People think you can’t be really sick if you aren’t very thin, insurance sucks, and the DSM still categorizes certain eating disorder diagnoses based on weight. In actuality, however, treatment is supposed to be geared towards the level of support people need for their eating disorders (see Fig. 3 for a brief explanation of the different levels). In-patient and Residential treatment are the highest levels of care and they serve to provide 24-hour care, provide medical stabilization, and symptom-use interruption with structured support before and after meals. In a perfect world, people would have the time, energy, and resources to go through each level of treatment at the pace that suits their own recovery journey, but that is not what happens. Insurance companies continue to refuse coverage for eating disorder treatment because there isn’t a one size fits all treatment for people. Insurance companies are leary to provide support if they aren’t confident in the research that emotional as well as behavioral and medical intervention are required to combat eating disorders (Kulkarni, 2012). This is a large reason why we often see (in movies, in real life, in media) people in medically low weights receive treatment disproportionately because there is present medical need. This leaves the MAJORITY of people struggling with eating disorders without the professional support they deserve.
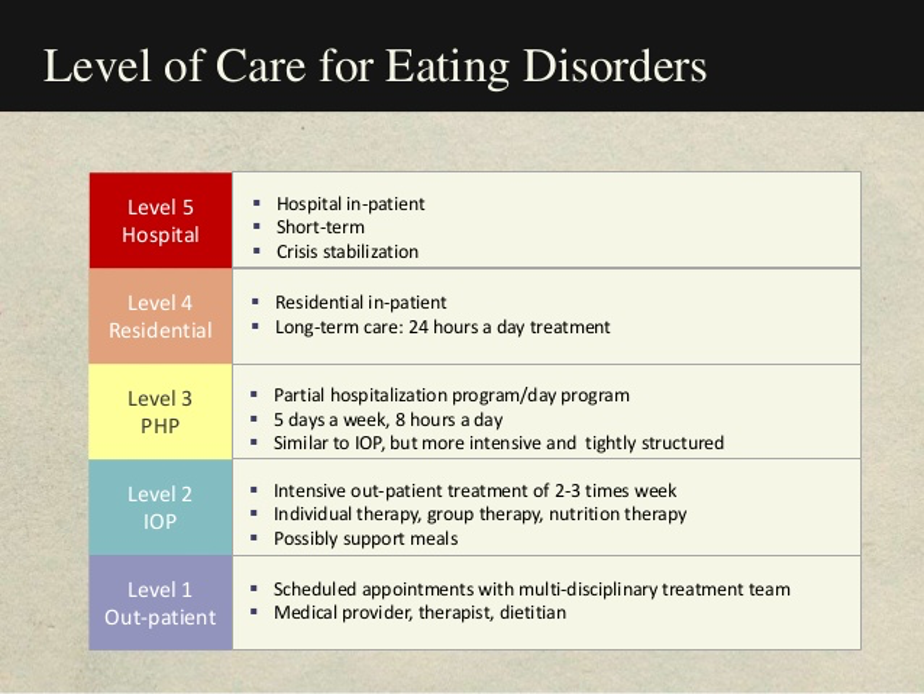
Figure 3. Levels of eating disorder treatment
Separating from my eating disorder will be all or nothing
Eating disorders serve a purpose. Those of us who suffer use them as a maladaptive tool to get needs met that we felt we couldn’t in other ways. People suffering can become so intertwined with their eating disorder, that it can feel like a part of them, a huge portion of their identity, if not the sole identity. That being said, when you embark on recovery, separating from it can be really challenging like losing an important relationship. You can, and it’s entirely normal to, grieve the loss of your eating disorder, and what it did for you. Wanting recovery does not require you to feel 100% excited. You can still work on recovery AND miss your eating disorder at the same time. Continuing with recovery, and developing your life outside of the eating disorder, overtime, can make that separation easier.
Once you regulate your eating behaviors you’ll be recovered
Eating disorders are not JUST about eating! People with eating disorders manipulate their relationship with food to cope. Often, this becomes the ONLY way to cope with any life stressors, so regulating eating behaviors means having to give up their most valuable coping mechanism. This can EXACERBATE feelings of anxiety, depression, irritability, and even make, you guessed it, eating disorder thoughts louder. Regulating eating behaviors is just the tip of the iceberg in recovery! In early recovery, success is often measured as how well one can comply with a prescribed meal plan. In later stages of recovery, people learn to regulate their own food choices and listen to their bodies.
Eating disorders are cured once someone does an inpatient treatment
False! This one is incredibly tough for several reasons. First and foremost, eating disorder treatment is BANANAS expensive! Insurance companies often base their coverage on weight (boo), which is an outdated and triggering practice. And if insurance is not an option, paying out of pocket gets expensive, quickly*. On average, the cost of residential eating disorder treatment is $956 per day in the U.S. (Frisch, et. al., 2006). So treatment may not even be an option for someone struggling with an eating disorder!
Secondly, this myth is closely related to the myth above. Eating disorder treatment is relatively short-lived, 45 days (~1.5 months) on average for a residential treatment program (Frisch, et. al., 2006). For about a month, patients are provided a structured environment to practice new coping skills, cease eating disorder behaviors, and receive emotional support. If insurance coverage allows, people will be able to step-down to the level of care that they need for their eating disorder (See Figure 3 above for the Treatment Step-Down process) After treatment (if applicable), people often have to go right back to the same triggering environment they used their eating disorder heavily in. So much work has to be done in that environment to make those new, more beneficial coping mechanisms stick. Recovery is incredibly hard, especially when one has to stay in the same environment with the same triggers that drove them to use the eating disorder in the first place. People deserve and REQUIRE external support at each stage of their recovery journey, in and OUT of treatment.
*check out our blog post: Insurance & Eating Disorder Treatment
References
“Eating Disorder Facts & Myths.” Eating Recovery Center, 2 Sept. 2020, www.eatingrecoverycenter.com/resources/eating-disorder-facts-myths.
Frisch, Maria J., et al. “Residential Treatment for Eating Disorders.” Wiley Online Library, John Wiley & Sons, Ltd, 9 Mar. 2006, onlinelibrary.wiley.com/doi/abs/10.1002/eat.20255.
Haines, Stephanie. “Are Eating Disorders A Choice?” Walden Eating Disorders, 10 Sept. 2018, www.waldeneatingdisorders.com/blog/are-eating-disorders-a-choice/.
Kulkarni, Shefali S. “Patients Often Find Getting Coverage For Eating Disorders Is Tough.” Kaiser Health News, 19 Oct. 2012, khn.org/news/binge-eating-disorder-insurance-coverage/.
Lauren Muhlheim, L., PsyD, CEDS. (2020, June 20). Eating Disorders in Transgender People. Retrieved February 22, 2021, from https://www.verywellmind.com/eating-disorders-in-transgender-people-4582520
Mortimer, Rose. “Pride Before a Fall: Shame, Diagnostic Crossover, and Eating Disorders.” Journal of Bioethical Inquiry, Springer Singapore, Sept. 2019, www.ncbi.nlm.nih.gov/pmc/articles/PMC6831528/.
Striegel-Moore, R. H. (1997). Risk factors for eating disorders. In M. S. Jacobson, J. M. Rees, N. H. Golden, & C. E. Irwin (Eds.), Annals of the New York Academy of Sciences: Vol. 817. Adolescent nutritional disorders: Prevention and treatment (p. 98–109). New York Academy of Sciences.
Strother, Eric, et al. “Eating Disorders in Men: Underdiagnosed, Undertreated, and Misunderstood.” Eating Disorders, Taylor & Francis, 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3479631/.